











































The 5As: A Practical Taxonomy for the Determinants of Vaccine Uptake
Sanofi Pasteur (Thomson); Kingston University (Robinson, Vallée-Tourangeau)
"Vaccine hesitancy may be due to a complex mix of behavioral and social factors, and most interventions to increase vaccine acceptance have shown little or no effect..."
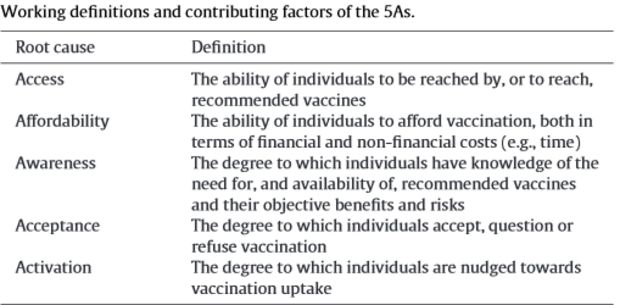
To develop a practical taxonomy to organise the myriad possible root causes of a gap in vaccination coverage rates, the authors of this study performed a narrative review of the literature and tested whether all non-socio-demographic determinants of coverage could be organised into 4 dimensions: Access, Affordability, Awareness, and Acceptance. Forty-three studies were reviewed, from which they identified 23 primary determinants of vaccination uptake. They identified a fifth domain, Activation, which captured interventions such as SMS [text messaging] reminders that nudge people towards getting vaccinated. The 5As taxonomy captured all identified determinants of vaccine uptake.
Only the following countries were included in the literature search: Estonia, Latvia, Lithuania, Brazil, Venezuela, Columbia, Peru, Bolivia, Argentina, Chile, Nigeria, Russia, India, Australia, United States (US), and United Kingdom (UK - England, Scotland, and Wales). Of the 38 studies included in the final sample, 15 studies focused on influenza (39%), 12 on measles, mumps, and rubella, or MMR (32%), 2 on diphtheria, pertussis (whooping cough), and tetanus (DTP)/DTP3, 1 on Hepatitis B, 2 on Bacille Calmette Guerin (BCG), 1 on Pneumococcal conjugate, 2 on childhood immunisations, and 2 on hepatitis B virus (HBV).
Studies classified under the access category (n = 13) revealed that access could be mediated by the place of birth, geographic allocation of the vaccination, impact of regular contact with the health care system, and convenience. Only 2 studies among the selected sample examined the impact of financial incentives on vaccine uptake. Three additional studies examined the impact of non-financial costs on vaccine uptake, with time costs as the most prominent non-financial affordability constraints. In terms of awareness, the most common reasons given by parents for failure to vaccinate were poor education and lack of knowledge about the vaccination schedule. Acceptance was the most commonly researched aspect of vaccine uptake. The acceptance factors identified pertained to the vaccine itself (n = 13), the disease it aims to protect individuals from (n = 8), individual characteristics (n = 12) like lack of trust, and the social context (n = 8) like peer influence. Two types of nudging techniques to boost activation were identified (n = 8): prompts and reminders as well as workplace policies. For example, in one study, children attending facilities with reminder systems in place were 5 times more likely to receive a flu vaccine, in comparison to healthcare facilities without these systems.
According to the authors, these findings suggest that, although there is a relationship between knowledge and acceptance, it is far from straightforward. This is consistent with many studies that have shown that provision of information and increased knowledge (awareness) may not change intentions or behaviours. In fact, while awareness and knowledge may be associated with an increase in acceptance among practitioners, it can actually mean a decrease in uptake in the general public. Another finding was that the most commonly studied predictors of vaccination uptake were related to acceptance. Factors included judgements about one's susceptibility to contract an infectious disease, the perceived severity of a contamination, as well as perceived benefits and judged efficacy of vaccination, concerns about side effects, and the impact of social norms. Using acceptance as a coding category also highlighted additional possible determinants such as trust, cognitive biases, and past behaviours.
While there is some ambiguity and possible overlap between the As for some factors, the 5As taxonomy has a very pragmatic objective: to facilitate the classification and characterisation of various possible determinants of a coverage gap by an inter-sectorial working group. This intuitive taxonomy has already facilitated mutual understanding of the primary determinants of suboptimal coverage in pilots in Europe, West Africa, and Latin America. These broader initiatives mobilise a cross-sector working group to analyse a gap in a vaccination programme, make a diagnosis, and then address it with targeted interventions.
"Future research may use this taxonomy to systematically compare and weight the importance of each of the 5As in explaining a vaccination gap for different vaccines or for one vaccine in different socio-cultural contexts. This in turn, would allow targeted, research-informed, interventions aiming to increase coverage rates."
Vaccine. 2016 Feb 17;34(8):1018-24 http://dx.doi.org/10.1016/j.vaccine.2015.11.065 - sent from Angus Thomson to The Communication Initiative on March 24 2016.
- Log in to post comments